Every morning, millions of people grab a bottle of mouthwash, swish for 30 seconds, spit, and feel clean.
It feels like the right thing to do. The burning sensation feels like it is killing something. The fresh mint taste feels like proof that it worked.
But what if that routine is actually making your mouth worse over time?
And what if the thing that actually works — oral probiotics — is sitting quietly on a health store shelf that most people walk right past?
This article is going to settle the debate properly. Not with opinions. With science.
We are going to look at exactly what mouthwash does, exactly what oral probiotics do, where each one works, where each one fails, and which one — or which combination — gives you the best long-term results.
First — What Problem Are We Actually Trying to Solve?
Before comparing two solutions, let us agree on what the problem is.
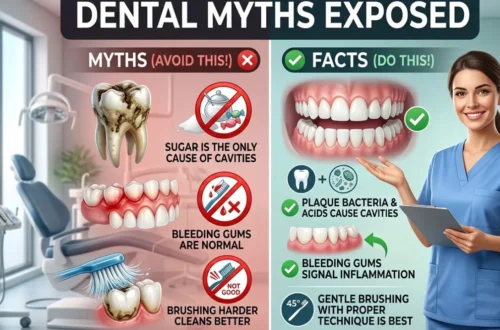
Your mouth contains over 700 species of bacteria. Some are essential and beneficial. Some are harmful and cause real damage — cavities, gum disease, bad breath, tooth loss.
The goal of any oral health intervention is simple: reduce harmful bacteria without destroying the beneficial ones.
That second part is the part most people forget. And it is exactly where the mouthwash vs probiotics debate becomes interesting.
Because these two approaches have completely opposite philosophies about how to reach that goal.
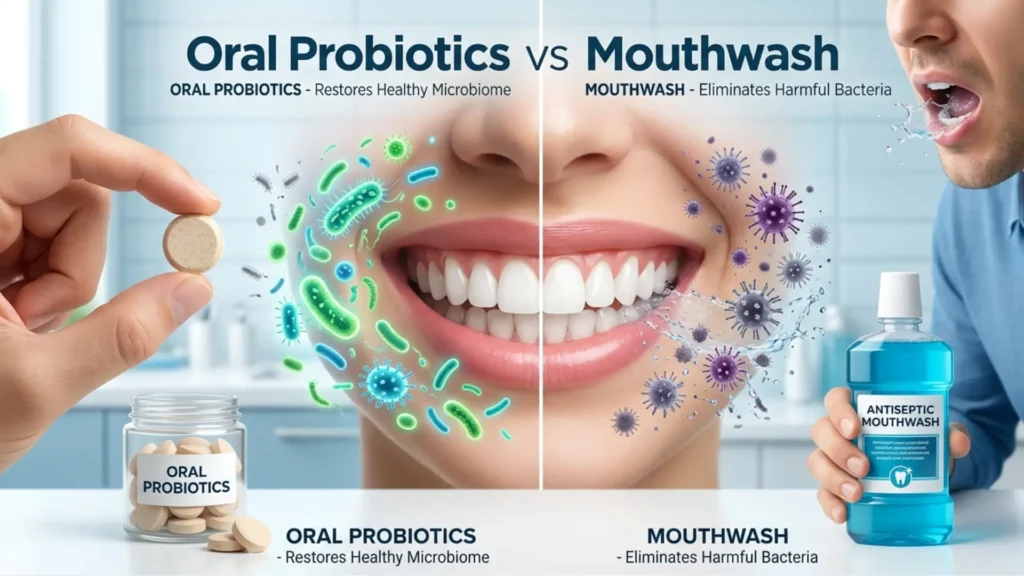
Mouthwash says: kill everything and start fresh.
Oral probiotics say: replace bad bacteria with good ones and restore balance.
One is a bomb. One is a garden.
Let us look at both honestly.
What Mouthwash Actually Does
Mouthwash has been around for over a century. Listerine — one of the oldest brands — was originally marketed as a surgical antiseptic and later as a floor cleaner before it became a mouth rinse. That history tells you something about how it works.
The Two Main Types of Mouthwash
Antiseptic / antibacterial mouthwash — This is the most common type. Ingredients like chlorhexidine, cetylpyridinium chloride (CPC), or essential oils (thymol, eucalyptol, menthol) work by killing or damaging bacterial cell membranes. They do not discriminate much between harmful and beneficial bacteria. They kill broadly.
Fluoride mouthwash — Works differently. It does not primarily kill bacteria. Instead it strengthens tooth enamel by incorporating fluoride into the enamel structure, making it more resistant to acid attack. Less controversial. More targeted.
Most over-the-counter mouthwashes — Listerine, Colgate, Oral-B — are antiseptic types. When people debate mouthwash vs probiotics, they are almost always talking about antiseptic mouthwash.
What Mouthwash Does Well
Let us be fair. Mouthwash has real benefits in the right context.
It reduces total bacterial count in saliva — measurably and quickly. Studies consistently show that rinsing with chlorhexidine or essential oil mouthwash immediately reduces the number of bacteria floating in your saliva by 75 to 99%.
It reaches areas brushing misses — the cheeks, roof of the mouth, back of the throat — areas that harbour bacteria contributing to bad breath.
It provides short-term fresh breath that lasts 1 to 3 hours depending on the product.
For specific situations — after oral surgery, during orthodontic treatment, or for patients with high infection risk — prescription-strength chlorhexidine mouthwash is genuinely clinically valuable.
Where Mouthwash Fails
Here is where it gets more complicated.
The effect is temporary. That 75 to 99% bacterial reduction lasts about 30 to 60 minutes. After that bacteria begin repopulating — from your tongue, your tonsils, your gums, your saliva. Within a few hours, counts are back to near-baseline. Swishing once a day produces one brief window of reduction. The rest of the day, bacteria do what they want.
It cannot reach biofilm bacteria. Plaque is not free-floating bacteria in your saliva. It is a structured colony — a biofilm — where bacteria are embedded in a protective matrix up to 1,000 times more resistant to antimicrobial agents than free-floating cells. Mouthwash kills the bacteria it touches in your saliva. It barely penetrates established plaque.
It kills beneficial bacteria too. This is the most underappreciated problem. Your mouth has a natural microbiome — a community of beneficial bacterial species that compete against harmful ones, produce antimicrobial compounds, and maintain a healthy pH. Antiseptic mouthwash does not distinguish between Streptococcus mutans (bad) and Streptococcus salivarius (beneficial). It kills both. Repeatedly using broad-spectrum antibacterial mouthwash disrupts the very ecosystem that naturally protects your mouth.
It may raise blood pressure with daily use. This finding surprised many people. A 2019 study in the journal Free Radical Biology and Medicine found that twice-daily use of antibacterial mouthwash significantly reduced nitric oxide production — a compound your body makes partly using beneficial oral bacteria. Nitric oxide helps regulate blood pressure. The study found that twice-daily mouthwash users had measurably higher blood pressure compared to non-users. This research is still developing but it has raised legitimate questions about daily antibacterial mouthwash use.
It does not address the root cause. Mouthwash reduces bacteria temporarily. It does nothing to change the underlying microbial environment of your mouth — the balance between harmful and beneficial species that determines your long-term oral health.
What Oral Probiotics Actually Do
Oral probiotics are a relatively new concept — at least as a commercial product. The science behind them has been building for about 20 years, but consumer products have only become widely available in the last 5 to 10 years.
The idea is fundamentally different from mouthwash.
Instead of trying to kill harmful bacteria, oral probiotics introduce specific strains of beneficial bacteria into your mouth. These beneficial strains then compete with harmful species for space and resources — crowding them out, producing antimicrobial compounds that suppress them, and gradually restoring a healthier microbial balance.
Think of your oral microbiome like a lawn. Harmful bacteria are weeds. Mouthwash is weedkiller — it clears everything temporarily but leaves bare soil that weeds quickly grow back into. Oral probiotics are grass seed — you fill the space with something beneficial so weeds have nowhere to establish.
The Key Oral Probiotic Strains
Not all probiotics are oral probiotics. Most probiotic supplements on shelves are designed for gut health — strains like Lactobacillus acidophilus or Bifidobacterium longum that survive stomach acid and colonize the intestine. These are not the same strains that colonize oral tissue.
Oral probiotics use strains that are specifically studied in mouth environments. The most important ones are:
Streptococcus salivarius K12 — The most researched oral probiotic strain in existence. Naturally found in the mouths of people with consistently good oral health and low bad breath scores. It produces powerful antimicrobial proteins called BLIS (bacteriocin-like inhibitory substances) — specifically lantibiotics M18 and B17 — that directly suppress S. mutans and the anaerobic bacteria responsible for bad breath. Multiple clinical trials show S. salivarius K12 significantly reduces volatile sulfur compound levels and bad breath scores.
Streptococcus salivarius M18 — A companion strain to K12. Produces different BLIS compounds with strong activity against S. mutans specifically. Shown in clinical trials to reduce cavity-causing bacteria and dental plaque formation.
Lactobacillus reuteri — Probably the most studied probiotic strain for gum health. Multiple clinical trials — including several randomized controlled trials — have shown that L. reuteri supplementation reduces gingival bleeding scores, reduces inflammatory markers in gum tissue, and lowers counts of key periodontal pathogens. A 2020 meta-analysis confirmed these findings across multiple independent studies.
Lactobacillus salivarius — Produces natural bacteriocins that target S. mutans specifically. Also shown to reduce P. gingivalis — one of the primary bacteria behind advanced gum disease.
Lactobacillus rhamnosus — Shown in studies with children to significantly reduce S. mutans counts and cavity rates when given regularly.
What Oral Probiotics Do Well
They address the root cause. Rather than temporarily reducing bacteria, oral probiotics change the composition of your oral microbiome over time. Consistent use gradually shifts the balance away from harmful species and toward beneficial ones. This is a sustainable long-term effect — not a 30-minute window.
They are selective. BLIS-producing strains like S. salivarius K12 specifically target harmful species. They do not indiscriminately kill everything. The beneficial microbiome remains intact and is actually strengthened.
They work where mouthwash cannot reach. Probiotic bacteria colonize oral tissue — the tongue, tonsils, gum tissue, and cheek lining. Once colonized, they produce their antimicrobial compounds continuously, 24 hours a day, in exactly the environments where harmful bacteria cause the most damage.
They provide lasting results. Studies show that regular oral probiotic use leads to sustained reductions in harmful bacteria — not just temporary suppression. One study found that S. salivarius K12 could be detected colonizing oral tissue for up to two weeks after a single course of supplementation.
The bad breath evidence is particularly strong. A double-blind randomized controlled trial published in the Journal of Applied Microbiology found that S. salivarius K12 supplementation reduced bad breath scores significantly over a 3-day period compared to placebo. Another study found an 85% reduction in bad breath episodes in participants taking S. salivarius K12 consistently. For chronic bad breath, the evidence for oral probiotics is stronger than for any mouthwash.
Where Oral Probiotics Have Limitations
They work slowly. You will not feel results in 30 seconds the way mouthwash seems to work. Building meaningful microbial colonization takes weeks of consistent use. Impatient users often give up before seeing results.
Consistency is essential. Unlike mouthwash which works on contact, oral probiotics need regular supplementation to maintain healthy populations. Stop taking them and the beneficial strains gradually decline.
Quality varies enormously. A probiotic pill designed for gut health does nothing for your mouth. You need oral-specific strains — particularly S. salivarius K12 and L. reuteri — in a form that delivers them to oral tissue, not the stomach. Lozenges and chewable tablets that dissolve in the mouth are far superior to swallowed capsules for oral health purposes.
The research, while strong, is still newer than the decades of evidence behind fluoride. More large randomized trials are still needed — particularly for specific clinical outcomes like cavity prevention and periodontal treatment support.
The Ultimate Guide to a Healthy Mouth and Oral Health (2026)
Head to Head — The Direct Comparison
| Comparison | Antiseptic Mouthwash | Oral Probiotics |
|---|---|---|
| Speed of action | Immediate (minutes) | Gradual (weeks) |
| Duration of effect | 30–60 minutes | Days to weeks with consistent use |
| Reaches biofilm? | Poorly | Yes — colonizes tissue directly |
| Kills beneficial bacteria? | Yes — non-selective | No — selective targeting |
| Bad breath | Temporary masking | Addresses root cause |
| Gum health | Limited long-term benefit | Strong clinical evidence |
| Cavity prevention | Temporary reduction only | Sustained reduction in S. mutans |
| Daily long-term use safety | Concerns emerging | Strong safety profile |
| Works below gumline? | No | Yes — colonizes gum tissue |
The Real-World Scenarios
Scenario 1 — You Have Chronic Bad Breath
Mouthwash: Gives you 1 to 2 hours of fresh breath. The mint covers the odor temporarily. Within hours the volatile sulfur compounds are back because the anaerobic bacteria producing them are still living on your tongue and below your gumline.
Oral probiotics: S. salivarius K12 colonizes your tongue and tonsils — exactly where bad breath bacteria live. It produces BLIS compounds that directly suppress them. Multiple studies show 85%+ reduction in bad breath with consistent use. Results take 2 to 4 weeks but they are real and lasting.
Winner: Oral probiotics — clearly.
Scenario 2 — You Just Had a Tooth Extraction or Oral Surgery
Mouthwash: Prescription chlorhexidine mouthwash is the clinical standard here for good reason. In the immediate post-surgical period, reducing total bacterial load quickly protects against infection. The broad-spectrum killing action is appropriate and necessary.
Oral probiotics: Not appropriate immediately post-surgery. You need rapid bacterial reduction, not gradual microbial rebalancing.
Winner: Mouthwash — clearly. This is its best use case.
Scenario 3 — You Want to Prevent Cavities Long-Term
Mouthwash: Fluoride mouthwash has genuine evidence here. Antibacterial mouthwash shows short-term reductions in S. mutans but no strong long-term cavity prevention data from daily use.
Oral probiotics: S. salivarius M18 and L. rhamnosus have shown sustained reductions in S. mutans counts and measurable reduction in cavity rates in clinical trials — particularly in children.
Winner: Oral probiotics for long-term prevention. Fluoride mouthwash as a useful complement.
Scenario 4 — You Have Gum Disease
Mouthwash: Chlorhexidine is used as an adjunct to professional treatment for gum disease. It helps short-term. But it does not address the biofilm below the gumline where periodontal pathogens live — and long-term chlorhexidine use has side effects including tooth staining and taste disturbance.
Oral probiotics: L. reuteri has the strongest evidence base here. Multiple clinical trials show measurable improvements in gum bleeding, pocket depth, and periodontal pathogen counts when added to standard professional treatment. A 2020 meta-analysis confirmed these benefits.
Winner: Oral probiotics as a long-term support tool. Professional treatment is still essential — both should be used.
Scenario 5 — You Just Want Fresh Breath Right Now
Mouthwash: Wins this one simply by being immediate. You have a meeting in 5 minutes. Mouthwash works right now.
Oral probiotics: Cannot compete with the immediate effect.
Winner: Mouthwash for instant, temporary freshness.
Should You Use Both?
Yes — but thoughtfully.
The key insight is that mouthwash and oral probiotics should not be used at the same time. If you swish with antiseptic mouthwash and then immediately take an oral probiotic lozenge, the mouthwash will kill the probiotic bacteria before they have a chance to colonize.
The smart protocol:
Use mouthwash in the morning if you choose to — before brushing or after, not immediately before taking probiotics.
Take oral probiotic lozenges at night — after brushing and before bed. This gives the probiotic strains the maximum opportunity to colonize oral tissue overnight when saliva flow is reduced and there is no food or drink to wash them away.
If you use chlorhexidine mouthwash, consider whether daily use is really necessary. Chlorhexidine is most appropriate for short-term therapeutic use — two to four weeks during a specific problem — not as a permanent daily habit. For daily maintenance, a fluoride rinse has a much better safety profile and can coexist with probiotics.
What About Natural Mouthwashes?
Some people switch to natural alternatives — oil pulling with coconut oil, diluted hydrogen peroxide, saltwater rinses, or herbal rinses containing ingredients like neem or tea tree oil.
Saltwater rinse — Genuinely useful for reducing inflammation and supporting healing after dental procedures. Not a substitute for regular oral hygiene but good for specific situations.
Oil pulling — Popular but weak evidence. Some small studies show modest reductions in S. mutans counts. No evidence it outperforms regular brushing. Fine as an add-on, not as a primary strategy.
Hydrogen peroxide — At diluted concentrations (1.5% or less) it can help with whitening and has some antibacterial effect. Like antiseptic mouthwash, it is non-selective. Not for daily long-term use.
Herbal rinses with neem or tea tree — Some antibacterial activity in laboratory studies. Less human clinical data than conventional mouthwashes or probiotics.
None of these natural options have the clinical evidence base that oral probiotics do for sustained oral microbiome improvement.
Choosing the Right Oral Probiotic Product
Since oral probiotic quality varies enormously, here is what to look for:
Strain specificity — The product should name specific strains, not just genus and species. Streptococcus salivarius K12 is specific. “Lactobacillus blend” is vague and unhelpful.
Delivery format — Lozenges, chewable tablets, or dissolvable strips that release in the mouth are far superior to swallowed capsules. You need these bacteria in your mouth, not your stomach.
Viable count — Look for products that guarantee viable bacterial counts at the time of use, not just at manufacture. Probiotics can die during storage. Reputable brands guarantee potency through the expiration date.
No unnecessary additives — Avoid products with artificial sweeteners that may themselves affect oral bacteria, or unnecessary fillers that dilute the active content.
One product worth mentioning is Provadent — which combines the key oral probiotic strains discussed in this article with complementary oral health ingredients including cranberry extract (for anti-adhesion effects against S. mutans). This kind of multi-mechanism formula makes scientific sense — probiotics restore beneficial bacteria while cranberry PACs simultaneously make it harder for harmful bacteria to colonize surfaces.
Frequently Asked Questions
Can I use mouthwash and oral probiotics together? Yes — but not at the same time. Space them apart by at least 2 to 3 hours. Ideally use mouthwash in the morning and oral probiotics at night after brushing.
How long do oral probiotics take to work? Most studies showing measurable results ran for 4 to 12 weeks of consistent use. Bad breath improvements from S. salivarius K12 can appear within 1 to 2 weeks. Gum health improvements from L. reuteri typically take 4 to 8 weeks.
Is daily mouthwash bad for you? Daily fluoride mouthwash — fine and beneficial. Daily antiseptic (antibacterial) mouthwash — increasingly questionable for long-term use. The emerging blood pressure data and concerns about disrupting the beneficial oral microbiome make daily antibacterial mouthwash less advisable as a permanent habit.
Do oral probiotics need to be refrigerated? Depends on the product and strains. Some oral probiotic strains are shelf-stable at room temperature. Others require refrigeration to maintain viability. Check the product label and follow storage instructions carefully.
Are oral probiotics safe for everyone? Oral probiotics have an excellent safety profile in research to date. Immunocompromised individuals should consult their doctor before using any probiotic product. For healthy adults and children, they are considered very safe.
Which is better for children — mouthwash or probiotics? For children, daily antiseptic mouthwash is generally not recommended by pediatric dentists. Fluoride mouthwash has appropriate use in cavity-prone children over age 6. Oral probiotics — particularly L. rhamnosus and S. salivarius strains — have strong safety and efficacy evidence in children for cavity prevention.
Does mouthwash help with gum disease? Chlorhexidine mouthwash is used as a short-term adjunct to professional gum treatment. It is not a long-term solution for gum disease on its own. Oral probiotics — particularly L. reuteri — have stronger evidence for long-term gum health support.
The Bottom Line
Mouthwash is not useless. It has real value in specific situations — post-surgical care, short-term therapeutic use, immediate breath freshening, and fluoride delivery to strengthen enamel.
But as a daily long-term oral health strategy, antibacterial mouthwash has serious limitations. It works for minutes. It kills beneficial bacteria alongside harmful ones. It does not address biofilm. And emerging evidence raises questions about its safety with unrestricted daily use.
Oral probiotics work differently — and for most long-term oral health goals, they work better. They address the root cause of bad breath, gum disease, and elevated cavity risk. They are selective. They colonize the exact environments where harmful bacteria do the most damage. And the evidence base — while newer — is consistently positive across independent research groups worldwide.
The smartest approach is not choosing one over the other. It is using each for what it does best — mouthwash for specific short-term situations, oral probiotics as your daily long-term investment in a healthier oral microbiome.
Your mouth is an ecosystem. Healthy ecosystems are not maintained by repeatedly bombing everything that grows in them. They are maintained by cultivating the right things to grow.
This article is written for informational and educational purposes only and does not constitute professional dental or medical advice. Please consult a licensed dentist or healthcare provider for diagnosis and treatment of any oral health condition.